At NovaVision we are often asked by clinicians and therapists to discuss the differences between NeuroEyeCoach and other saccadic training programs – both those which appear to be specifically for saccadic training and those which have a saccadic training module within a therapy training suite of programs.
A lot of clinical data over the years¹ has demonstrated that neurological rehabilitation cannot be safely guided and aided by non-specific, unsupervised interventions:
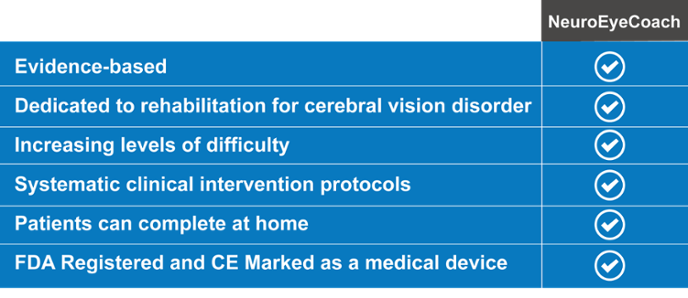
- Intervention should be evidence based, supported by rigorous research and clinical data.
- Intervention should be designed specifically for a clinical condition, and should not try and address either multiple conditions or general conditions.
- Intervention should be supervised or self-adaptive with systematically developed protocols, as changes in brain-based healing that benefit one person may be detrimental to another.
These criteria are at the heart of the difference between NeuroEyeCoach and other saccadic or general therapy training programs, and of key importance for clinicians and other assessing available alternatives.
Evidence Based
NeuroEyeCoach is underpinned by the fundamental concept of evidence-based medicine and was developed based on the findings of 13 empirical studies covering 551 patients with homonymous visual field loss and persistent visual disabilities². Each aspect of the program is supported by the findings of one of the 13 studies. The main outcome of saccadic training demonstrated in these studies is a significant improvement in visual search performance accompanied by more efficient oculomotor strategies, and a reduction in visual disability as assessed by standardized questionnaires and behavioral measures. These include measures of improvements in navigation skills and object finding. The efficacy of this treatment approach to improvement of visual overview and visual exploration is superior to practice with reading, non-specific visual training, standard occupational therapy or counseling with regards to coping strategies. Importantly, time since brain injury and age of hemianopic patients do not play a significant role in the treatment effect.
Designed for Purpose
A recent multi-center study specifically on NeuroEyeCoach published in BioMed Research International³ stated: “Other than [the use of visual search] in various forms in a limited number of rehabilitation clinics over the past 25 years, there has been a marked lack of availability of an effective evidence-based gold-standard registered medical device accessible to patients at home or in clinical settings. In clinical practice, the void has been filled by the use of a number of devices that originally had been designed to address other problems, hence being sub-optimum for the rehabilitation of vision loss”.
Programs that were originally designed for a different purpose, such as improving athletes’ performance on visuo-motor tasks, are not able to dissociate perceptual problems from those of limb function deficit; this makes it difficult to assess how much of the change in behavior is due to better visual scanning versus motor coordination. Similarly, programs that address more than one condition that really require specific interventions, such as vision and reading, can confuse treatment and lead to sub-optimal outcomes. Finally, saccadic programs that are merely a module in a broad suite of programs are not able to provide the level of systematic intensity and patient engagement that is possible with a dedicated program.
NeuroEyeCoach is not aimed at producing non-specific general effects, but very specifically designed to target visual disorders resulting from neurological brain damage. Through the provision of a personalized therapy covering 36 progressive stages over a 2-4 week period, NeuroEyeCoach is designed to help improve scanning and eye movement efficiency in patients with homonymous visual field loss. It does not try to address any other clinical issue.
Systematic Protocols
An effective training program requires a set of systematically developed protocols, specific to neurologically visually impaired patients, to induce change and monitor progress. Alternative programs do not provide a specific plan for the management of patients or systematic protocols for the physician to change task difficulty. As a result physicians are required to devise tests and there are no reliable measures of improvement provided.
NeuroEyeCoach is a systematic program that has multiple layers of difficulty and which is self-adaptive, adjusting to the patient’s needs and stage of recovery. The program is personalized to the patient from the outset and by adapting to the patient’s progress the task difficulty is altered to encourage improvement; conversely, should the task be too difficult, it is automatically modified to avoid fatigue and despondency. The criterion for success is also automated to ensure a standardized measurement. The program provides software-guided training steps, eliminating any need for ad hoc improvisation; it is therefore not subject to “physician interpretation” but does benefit from “physician supervision”.
Conclusion
While other programs may have merit in their own right however as they relate to vision they are not evidence based and not specifically designed to target scanning and eye movement efficiency in patients who have experienced visual disorders from brain damage; they also lack standardized measurements based on systematic protocols. A final key advantage for NeuroEyeCoach is its flexible delivery; patients can start the program while in a clinical environment and then complete it at home.
1. See interview with Dr. Alvaro Pascal-Leone
2. For details on and links to these studies, go to the-science-behind-neuroeyecoach/
